In 2008, 60% of unintended pregnancies resulted in birth, while 40% ended in abortion. The abortion debate has been traditionally very polarizing and carries moral undertones. Recently, discussions surrounding when a prenatal infant experiences pain has resulted in policies similar to this one surfacing at state and federal levels (ex. H.R.36 -114th Congress).
Scope of Issue
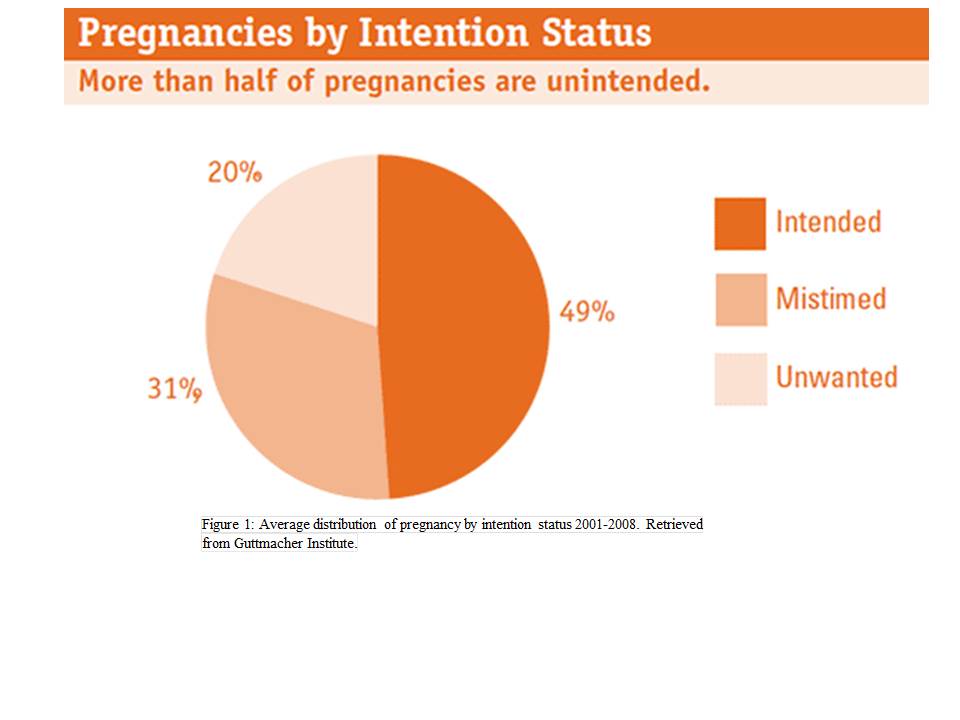
According to the Guttmacher Institute (2015), each year in the United States over 50% of pregnancies are unintended. This issue overly affects poor and low-income women (more than 5x the rate of high-income women) and can result in poor health outcomes for both women and their children.
Summary of the Act
A pregnant woman can receive an abortion in the state of Ohio if…
- The unborn child is less than 20 weeks post-fertilization
- In order to prevent the death of the pregnant woman
- In order to prevent “substantial and irreversible damage” or bodily impairment of the pregnant woman
If a pregnant woman wishes to receive an abortion…
- Physicians must document, in writing, their reasons for performing an abortion of an unborn child over 20 weeks and must receive approval from a second, unrelated physician.
- Abortion must occur where neonatal/premature infant health care services are available.
- The physician is required to select and cite, in writing, methods of abortion that creates the best opportunity for the unborn child’s survival, unless it poses greater risk for the woman.
- Lastly, one other physician must be present when the abortion is performed; their purpose is to take all necessary precautions to save the life of the unborn child post-abortion.
Critiques
Requiring secondary approval from another physician can be viewed as both a strength and a weakness as it can result in delay in procedure, posing a greater health risk in cases where maternal health is in jeopardy, or it can allow women to get a second opinion of their health outcomes. Additionally, in certain areas of the United States, access to facilities where adequate prenatal care services are available may result in decreased accessibility to abortive services. Low-income, at-risk women often live in these areas, which lack access to certain specialized health care services. Therefore, the populations of women who are more likely to seek abortive services are least likely to gain access to these resources. Furthermore, the act takes into consideration the physical health concerns, but not the mental health concerns affecting the pregnant woman, such as in incidences of rape or incest.
Recommendations
It is essential to accompany this act with more funding for community-based agencies which provide financial, health, birth control, and other supportive services to women encountering an unintended pregnancy that wish to carry their unborn child to full-term, which might be their only option due to this act. If restrictions are being placed on women’s access to abortions, then we must provide them with support for the health of both woman and unborn child and the financial stability of the woman. Culturally, we must continue to decrease the stigma surrounding unintended pregnancies and increase paternal involvement in these cases as well.