
Complexity Reduction for Cyber-Physical-Human Medical Systems
As computing devices deeply and pervasively affect our daily lives, new requirements arise for the seamless integration of physical objects and computing systems. Cyber-physical systems (CPS) are systems that tightly combine physical elements and computation resources through communication technologies. For medical systems, human factor plays an extremely important role, since medical decisions, such as diagnoses and treatment plans, are rely on medical staff. In this work, we focus on the complexity and safety issues of medical Cyber- Physical-Human Systems (CPHS). A report from Institute of Medicine (IOM) suggested that medical errors cause about between 44,000 and 98,000 preventable deaths and 1,000,000 excess injuries each year in hospitals. In order to improve safety of healthcare, Medical Device Plug-and-Play (MDPnP) was proposed to collect and consolidate medical information, and allows the reconfiguration of medical devices. We argue that such an integrated infrastructure opens a door for reducing preventable safety hazards, but it also significantly increases the complexity of the system due to the interactions of devices, controllers, patients and medical staff. Without properly controlling and reducing complexity, systems with high complexity may even cause more safety hazards. As National Science Foundation has remarked, “These advances have not only made it possible to reach the frontier faster; they have also increased by orders of magnitude the levels of complexity open to exploration and experimentation. Understanding complexity and learning how best to harness these new capabilities are both a challenge and a responsibility.”
From a computer science perspective, complexity reflects the workload of performing tasks by measuring number of steps or elapsed time. In this work, we examine complexity from a safety angle, identify three major types of complexity, and propose complexity reduction and control mechanisms to address them. Followings are different types of complexity. First, verification complexity, in terms of model checking state space, is one of the major aspects must be addressed. Formal verification is a promising technique to guarantee correctness and safety, but the high interactive complexity of the system components significantly increases the verification cost, which is known as state space explosion problems.
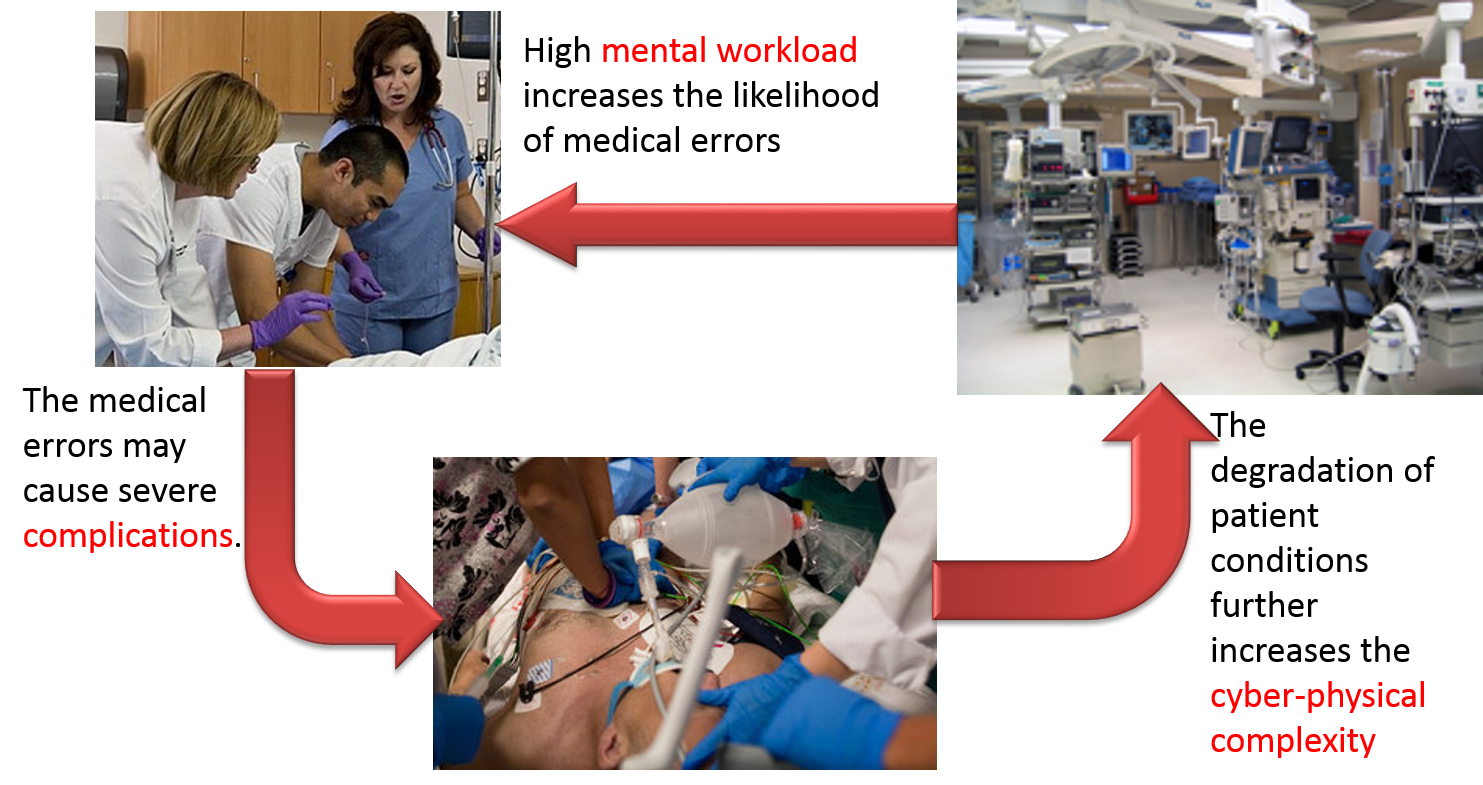
Second, cyber medical treatment complexity is another essential aspect. Cyber medical treatment complexity is defined as the number of steps and time to perform a treatment and monitor the corresponding physiological responses. Several steps are generally involved to perform a treatment, including deciding the best fit treatments, checking preconditions, administering, monitoring side effects, and checking expected responses. However, in an intensive care unit (ICU), patients are seriously ill, and there is often short of time and short of information for medical staff to make decisions. Moreover, medical staff are under tremendous pressure and overloaded by the great amount of unorganized information.
Third, mental workload complexity must be addressed as well. Mental workload complexity measures human memory and mental computation demand for performing tasks. In the current medical practice, medical staff are usually overwhelmed by the great amount of unorganized physiological data. In addition, the current display systems lack of medical context-dependent information, such as workflows, to assist medical staff to follow the best practice medical guidelines.
We need new breed of system architecture designs, which include architectural design patterns and protocols, to reduce and control the complexity of medical cyber-physical-human systems. We have addressed part of the problems by proposing architectural patterns for consistent coordination and validation with low complexity. Furthermore, the complexity issues become even more challenging when human is involved in the control loop, and we will address the human factor in the remaining work. The main objectives of this work are to 1) reducing verification complexity by proposing new reference architectural patterns that can guarantee consistent coordination; 2) reducing cyber medical treatment complexity by proposing a treatment validation protocol; 3) reducing mental workload complexity by improving situation awareness and preventing deviation from the best practice medical guidelines if possible.
Publications
- Heechul Yun, Po-Liang Wu, Maryam Rahmaniheris, Cholgi Kim, and Lui Sha. 「A reduced complexity design pattern for distributed hierarchical command and control system」. International Conference on Cyber Physical System (ICCPS). April, 2010 (paper)
- Po-Liang Wu, Woochul Kang, Abdullah Al-Nayeem, Lui Sha , Richard Berlin, Julian Goldman. 「A Low Complexity Coordination Architecture for Networked Supervisory Medical Systems」. International Conference on Cyber Physical System (ICCPS). April, 2013 (paper, slides)
- Woochul Kang, PoLiang Wu, Maryam Rahmaniheris, Lui Sha, Richard B. Berlin Jr.,Julian M. Goldman, 「Towards Organ-Centric Compositional Development of Safe Networked Supervisory Medical Systems」, The 26th IEEE International Symposium on Computer-Based Medical Systems (CBMS 2013), June, 2013 (paper, slides)
- Po-Liang Wu, Dhashrath Raguraman, Lui Sha, Richard Berlin, Julian Goldman 「A Treatment Validation Protocol for Cyber-Physical-Human Medical Systems」. to appear in EUROMICRO Software Engineering and Advanced Application (SEAA) 2014
- Po-Liang Wu, Lui Sha, Richard Berlin, Julian Goldman, 「Safe Workflow Adaptation and Validation Protocol for Medical Cyber-Physical-Human Systems」, to appear in EUROMICRO Software Engineering and Advanced Application (SEAA) 2015
Presentation